Hemorrhoids
What is Hemorrhoids?
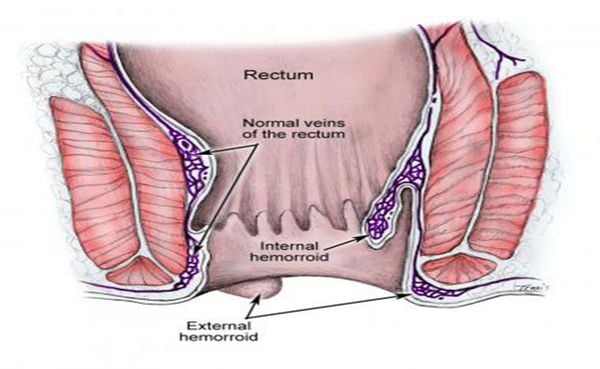
Hemorrhoids, also called piles, are swollen veins in your anus and lower rectum, similar to varicose veins. Hemorrhoids can develop inside the rectum (internal hemorrhoids) or under the skin around the anus (external hemorrhoids).
Risks to develop hemorrhoids
So far, the causes of haemorrhoids are unknown. However, risk factors are identified as following:
- Straining during bowel movements
- Sitting for long periods of time on the toilet
- Having chronic diarrhoea, obstructed defecation or constipation
- Being obese
- Being pregnant
- Having anal intercourse
- Eating a low-fiber diet or too much hot, spicy food
- Regular heavy lifting or sedentary lifestyle
Pathophysiology
- the theory of varicose veins: haemorrhoids were caused by varicose veins in the anal canal
- the theory of sliding anal canal lining: haemorrhoids develop when the supporting tissues of the anal cushions disintegrate or deteriorate
Symptoms
- Painless bleeding during bowel movements. You might notice small amounts of bright red blood on your toilet tissue or in the toilet.
- A haemorrhoid to push through the anal opening (prolapsed or protruding haemorrhoid), resulting in pain and irritation.
- Pain, Severe pain or discomfort
Classification
- Internal Haemorrhoids
- External Haemorrhoids
- Mixed Haemorrhoids
Diagnosis
- Internal Hemorrhoids:
A first-degree internal hemorrhoid bulges into the anal canal during bowel movements.
A second-degree internal hemorrhoid bulges from the anus during bowel movements, then goes back inside by itself.
A third-degree hemorrhoid bulges from the anus during bowel movements and must be pushed back in with a finger.
A fourth-degree hemorrhoid protrudes from the anus all the time.
-External haemorrhoids: hemorrhoid protrudes from the anus all the time
-Mixed haemorrhoids: including internal and external haemorrhoids
Treatment
Non-surgical treatment:
More than 90% of patients with haemorrhoids are treated by non-surgical treatment, including internal medicine treatment and procedures
Advantages:
- No pain
- No hospitalization
- Avoid surgery
Drawback: poor result with haemorrhoids at the late stages (Stage 3 and 4)
Internal medicine treatment:
- Change the diet and lifestyle: provide more fiber and water; reduce hot, spicy food. Being active and exercise. Avoid sitting for too long.
- Medicine: Increase the protection of vascular walls, prevent constipation
Therapeutic indications:
- Highly effective for haemorrhoids at early stages (stage 1 and 2), supportive effect for haemorrhoids at late stages (stage 3 and 4)
- Preventive treatment for haemorrhoids.
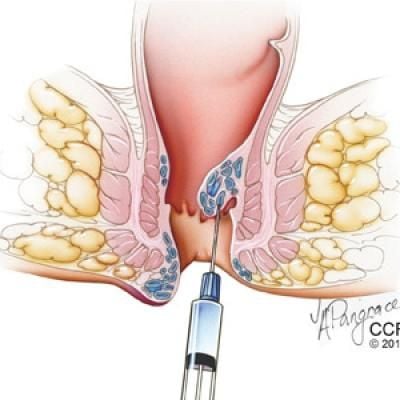
Procedure:
- Sclerotherapy with guidance of Doppler ultrasound
Therapeutic indications: Haemorrhoids stage 1, 2 and 3, 4 (single pile) or non-surgical contraindication cases.
- Rubber band ligation
Therapeutic indications: Internal haemorrhoids stage 1, 2 and 3 (small single pile)

Surgical treatment:
Less than 10% of patients with haemorrhoids are undergone surgery, including:
- Cases that are at late stages (Stage 3, 4 or complication)
- Cases that are failed with non-surgical treatment
* Advance surgical techniques:
Transanal Hemorroidal Dearterialization guided by Doppler ultrasound is an advance surgical technique with minimal invasion due to the principle: the hemorrhoidal arteries are identified by Doppler ultrasound, then a suture ligation is performed to effectively decrease the blood flow to the hemorrhoidal plexus. In case of redundant prolapse, the prolapsed mucosal membrane is lifted and sutured, repositioning hemorrhoidal cushions in situ.
In this technique, there is no tissue excision, no incisions, and maximising the protection of anorectal canal structure. Therefore, post-operative pain is minimized for patients, hospitalized period is shortened (24 hours) and patients are able to come back to normal work quickly.
Therapeutic indication: Internal haemorrhoids stage 1,2,3,4. The technique could also be applied in case of anal fissure, papilloma condylome, vascular occlusion…
Longo surgery:
Principle: Using an adapted circular stapler to excise a mucosal cylinder and lower the rectual mucous membrane, aiming at revascularize the cushions.
However, the anal recto associations of USA and Europe recommend that Longo technique is indicated only for haemorrhoids with circumferential ring.
* Classic surgical techniques with or without power: radio, laser…
- Milligan-Morgan opened surgery
- Ferguson closed surgery
Indication: Haemorrhoids stage 3, 4, vascular occlusion, or Cases that are failed with non-surgical treatment
Recurrence
So far, there are no treatment solutions with zero percent of recurrence. In general, the rate of recurrence is approximately under 15%. By that it means more than 85% of the cases were not recurrent of haemorrhoids.
In conclusion: For patients with haemorrhoids, non-surgical treatments have higher rate of recurrence compared to surgical treatments. However, non-surgical treatments avoid a surgery and the treatment could be re-applied when facing recurrence.
